|
Laparoscopic Roux-en-Y Gastric Bypass
|
|
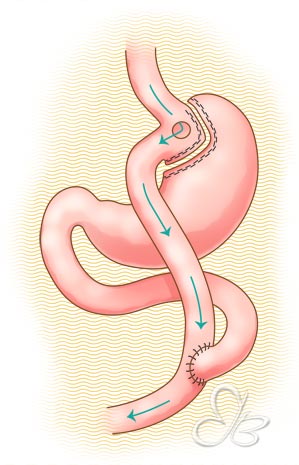
This procedure combines elements of both restriction and malabsorption.
|
|
A small pouch of upper stomach (approximately 25mls volume) is partitioned and separated from the rest of the stomach using surgical staplers. This small volume gastric pouch severely restricts food intake, one of the mechanisms for weight loss in this procedure.
|
|
Food is then routed through a ‘Roux’ limb of small intestine before being allowed to come into contact with digestive (bile & pancreatic) secretions much further downstream than normal. The food stream effectively bypasses most of the stomach and part of the upper small intestine, causing a certain degree of malabsorption and reducing the amount of calories and nutrients absorbed.
|
|
If you have problems with portion control, gastric bypass may be a good option for you. The small stomach pouch prevents overeating. When patients eat more than the pouch can hold, they experience abdominal discomfort and may throw up.
|
|
Gastric bypass causes a fall in levels of the hunger-stimulating hormone, Ghrelin. Consequently, although gastric bypass patients eat very small portions, they do not experience the hunger pangs and food cravings that dieters complain about: life no longer revolves around food!
|
|
Gastric bypass may also be a good option for people who have trouble controlling sweet intake. In about 40% of patients who have had gastric bypass, a sugary meal/drink causes a phenomenon known as 'dumping syndrome'. Symptoms of dumping syndrome include dizziness, sweating, palpitations, nausea, abdominal cramps and diarrhea – these symptoms begin 10 – 60 minutes after patients have their sugar fix. This feature of gastric bypass is considered desirable because it forces behavior modification, basically 'training' sugar junkies to avoid soda, sweets, candy, chocolate and ice cream.
|
- This operation is reversible. However, surgically reversing a gastric bypass is a technically demanding procedure
- It does not involve placement of an implant
- It does involve cutting/stapling of the stomach and rerouting or rearrangement of the intestines in order to cause some degree of malabsorption. There is therefore a risk of developing nutritional deficiencies such as iron, calcium and vitamin deficiencies. Gastric bypass patients must agree to take long-term nutritional supplements
- It is considered to have a higher surgical risk compared to sleeve gastrectomy and gastric banding
- The average hospital stay following this procedure is between 3 – 5 days
- Gastric bypass is associated with excellent weight loss: on average patients lose 65 – 75% of their excess weight
- Gastric bypass has been performed for over 50 years and therefore has a proven record as a bariatric procedure producing durable, long-term weight loss
|